Patients at Increased Risk of PAD:
•Age ≥65 y
•Age 50–64 y, with risk factors for atherosclerosis (eg, diabetes mellitus, history of smoking, hyperlipidemia, hypertension) or family history of PAD (52)
•Age <50 y, with diabetes mellitus and 1 additional risk factor for atherosclerosis•Individuals with known atherosclerotic disease in another vascular bed ( eg, coronary, carotid, subclavian, renal, mesenteric artery stenosis, or AAA)
•Individuals with known atherosclerotic disease in another vascular bed ( eg, coronary, carotid, subclavian, renal, mesenteric artery stenosis, or AAA)
History and/or Physical Examination Findings Suggestive of PAD:
History
•Claudication
•Other non–joint-related exertional lower extremity symptoms (not typical of claudication)
•Impaired walking function•Ischemic rest pain
Physical Examination
•Abnormal lower extremity pulse examination
•Vascular bruit
•Nonhealing lower extremity wound
•Lower extremity gangrene
•Other suggestive lower extremity physical findings (eg, elevation pallor/dependent rubor)
In patients at increased risk of PAD but without history or physical examination findings suggestive of PAD, measurement of the resting ABI is reasonable (IIa)
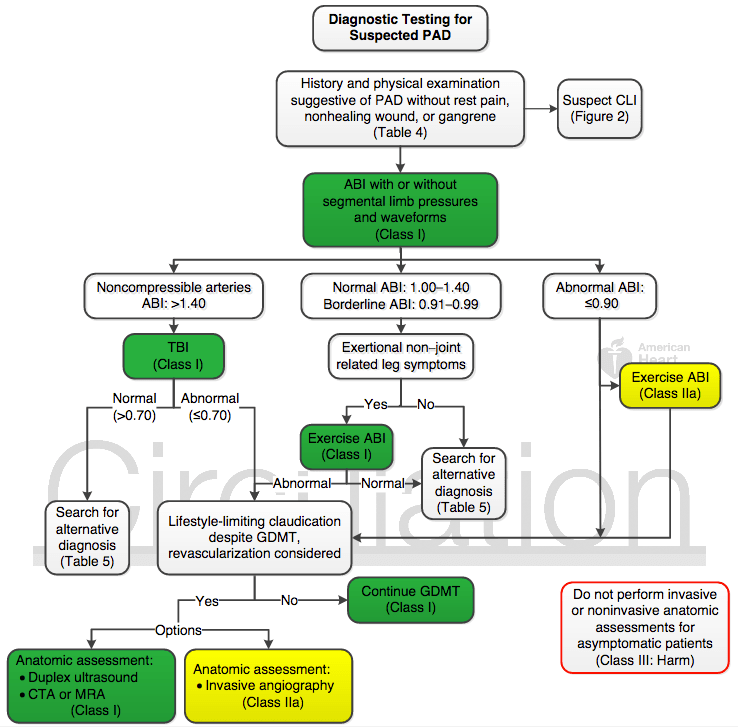
Diagnostic Testing for PAD

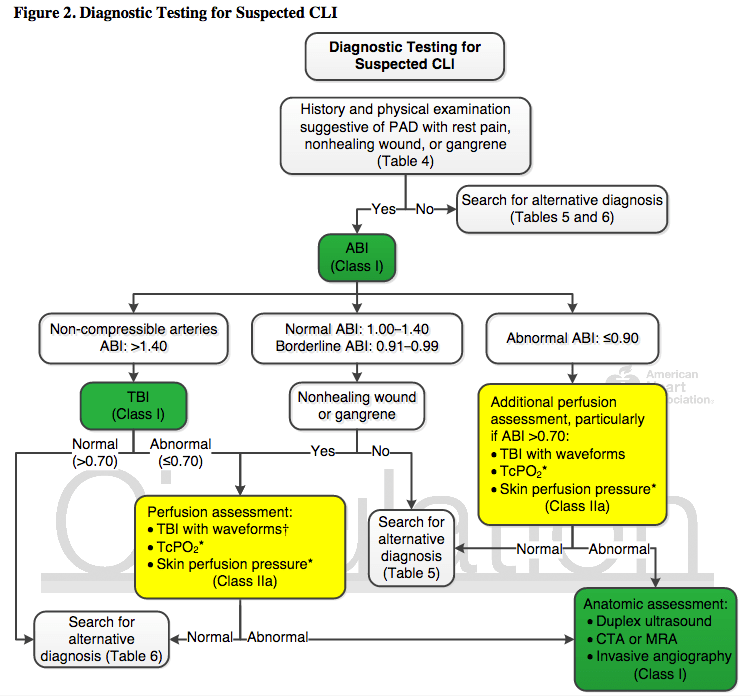
Diagnostic Testing for CLI
Medical therapy:
Diagnostic Testing for CLI
Medical therapy:
•Start Aspirin (75 – 325 mg daily) alone or clopidogrel (75 mg daily) in symptomatic PAD or asymptomatic PAD with ABI ≤0.90
•DAPT may be reasonable after revascularization
•High-intensity statin
•Antihypertensive therapy, preferably with ACE inhibitor or ARB
•Smoking cessation counseling and therapy as well as referral to smoking cessation program
•Glycemic control
•Cilostazol to improve symptoms
•Influenza vaccination
•Structured exercise therapy
•Counseling for self-foot examination as well as prompt diagnosis and treatment of foot infection
Revascularization:
•Revascularization is a reasonable option for patients with lifestyle-limiting claudication and hemodynamically significant aortoiliac or femoropopliteal disease
•In patients with CLI, revascularization should be performed when possible to minimize tissue loss (irrespective of location)
•Patients with PAD who have undergone lower extremity revascularization (surgical and/or endovascular) should be followed up with periodic clinical evaluationandABImeasurement.
Additional Screening:
•Abdominal aortic aneurysm
•Do NOT screen for coronary, carotid or renal disease
Reference:
