Significant Changes Compared to 2013 Heart Failure Guidelines:
- Screening for heart failure with BNP acceptable for patients hypertension, diabetes mellitus, or known vascular disease. Patients with BNP > 50 ng/mL should undergo further evaluation with echocardiography and referral to a cardiologist (Class of recommendation – IIa)
- A pre-discharge BNP is appropriate to evaluate post-discharge prognosis (Class of recommendation – IIa)
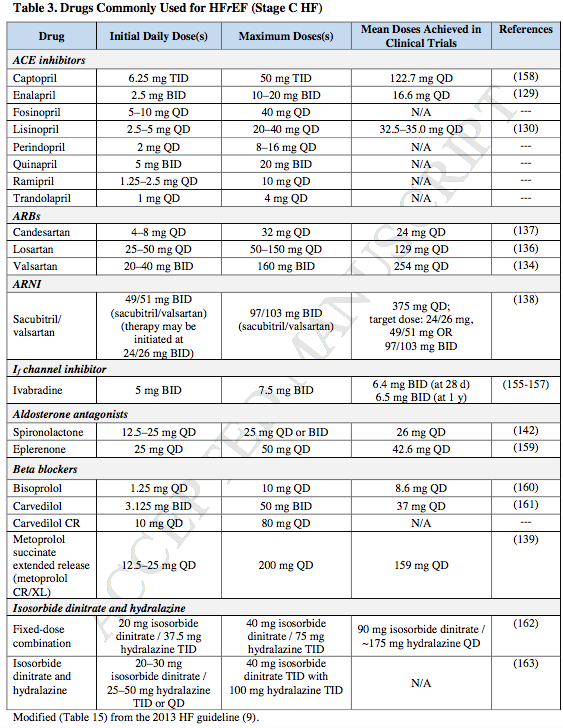
- As in the table above, ACE replacement by an ARB + ARNI is recommended (Class of recommendation – I)
- As in the table above, Ivabradine in addition to a beta-blocker to achieve a heart rate of < 70 bpm (Class of recommendation – IIa)
- In patients with NYHA class II and III HF and iron deficiency (ferritin <100 ng/mL or 100 to 300 ng/mL if transferrin saturation is <20%), intravenous iron replacement might be reasonable to improve functional status and quality of life (Class of recommendation – IIb)
- In HFrEF as well as HFpEF, aim for systolic blood pressure < 130 mmHg (Class of recommendation – I)
- Based on data from TOPCAT, an aldosterone receptor antagonists might be considered in HFpEF (EF ≥ 45 %) to decrease hospitalizations
Ref: 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure. Clyde W. Yancy, Mariell Jessup, Biykem Bozkurt, Javed Butler, Donald E. Casey, Monica M. Colvin, Mark H. Drazner, Gerasimos S. Filippatos, Gregg C. Fonarow, Michael M. Givertz, Steven M. Hollenberg, JoAnn Lindenfeld, Frederick A. Masoudi, Patrick E. McBride, Pamela N. Peterson, Lynne Warner Stevenson, Cheryl Westlake. Journal of the American College of Cardiology Apr 2017, 23682; DOI: 10.1016/j.jacc.2017.04.025